RECURRENT SHOULDER DISLOCATION
The shoulder joint is a ball-and-socket joint, formed by the head of the humerus (ball) and the glenoid cavity (socket)of the scapula. It is the most mobile joint in the human body, but this mobility also makes it prone to instability

How long is recovery from shoulder arthroscopy?
Stabilizers of the Shoulder Joint
Shoulder stability is maintained by two types of stabilizers:
- Static Stabilizers (non-contractile structures)
- Glenohumeral ligaments (SGHL, MGHL, IGHL)
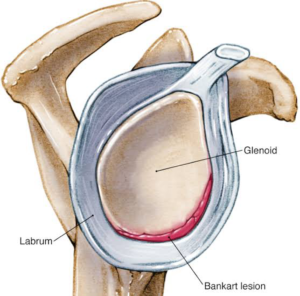
- Glenoid labrum – Deepens the socket by 50%
- Articular congruity and version – Helps maintain stability
- Negative intra-articular pressure – Creates a suction effect
- Joint capsule – A soft tissue stabilizer
- Rotator interval – Connects supraspinatus and subscapularis
- Dynamic Stabilizers (muscles)
- Rotator cuff muscles – Compress humeral head against the glenoid
- Biceps long head – Acts as a humeral head depressor
- Periscapular muscles – Assist in shoulder movement
Glenohumeral Ligaments (GHL) and Their Role
Superior Glenohumeral Ligament (SGHL)
- Origin: Anterosuperior glenoid labrum (12–1 o’clock position)
- Function: Prevents downward movement of the humeral head in neutral rotation
Middle Glenohumeral Ligament (MGHL)
- Origin: 2–3 o’clock position on the glenoid
- Function: Restricts external rotation and forward movement of the humerus at 45° abduction
Inferior Glenohumeral Ligament (IGHL)
Has two bands:
- Anterior Band – Prevents forward dislocation; weak link in Bankart lesions
- Posterior Band – Prevents backward dislocation; tightness can cause SLAP lesions
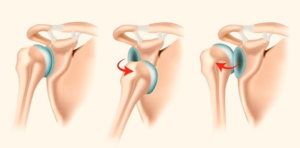
Shoulder Instability
Types of Shoulder Instability
- Unidirectional – Anterior (most common), Posterior, Inferior, or Superior
- Multidirectional – Due to structural changes or muscle weakness
Anterior Shoulder Instability & Bankart Lesion
Bankart Lesion
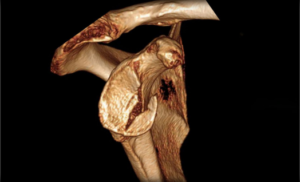
Bony Bankart Lesion
Hill-Sachs Lesion
- Impression fracture of the humeral head due to dislocation
- Large lesions may cause recurrent dislocations

Grading Shoulder Instability
Grade
Translation of Humeral Head
0
Normal movement
1
Up to the glenoid rim
2
Over the glenoid rim but reduces spontaneously
3
Dislocates and does not reduce
Symptoms of Shoulder Instability
- Recurrent dislocations
- Pain with overhead movements
- Feeling of instability or shoulder “popping out”
- Dead arm syndrome (sudden numbness and weakness)
Physical Examination Tests
- Load and Shift Test
- Assesses anterior and posterior stability by applying force to the humeral head
- Apprehension Sign
- Patient lies supine, arm abducted and externally rotated
- Feeling of impending dislocation indicates instability
- Relocation Test
- Similar to apprehension test but with posterior pressure applied
- Reduction in apprehension confirms anterior instability
- Sulcus Sign
- Inferior traction on the arm
- Dimpling below acromion suggests inferior instability
- Drawer Test
- Assesses anterior/posterior humeral translation
Diagnostic Imaging
X-rays
- AP, Axillary, and Scapular Y views
- Hill-Sachs lesion (Stryker Notch view) and Bony Bankart lesion (West Point Axillary view)
MRI & MR Arthrography
- Best for detecting labral tears and soft tissue injuries

CT Scan
• Best for evaluating bony defects (Bony Bankart, Hill-Sachs lesions)
Treatment of Shoulder Instability
Non-Surgical Treatment
• Immediate reduction followed by immobilization (1 week max) & physiotherapy
• High risk of recurrence in young athletes (<20 years, males, contact sports, hyperlaxity, >20-25% glenoid bone loss)
Surgical Treatment
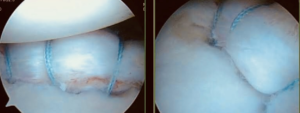
1. Arthroscopic Bankart Repair (Preferred)
• For athletes <25 years with a Bankart lesion
• Minimally invasive, better outcomes than open surgery
- Bankart Repair + Remplissage
- Latarjet (Coracoid Transfer) or Bristow Procedure
Conclusion
Dr. Nitin Rawal and his team provide the best shoulder treatment in Gurgaon, offering expert care for shoulder injuries and instability with advanced surgical and non-surgical techniques.