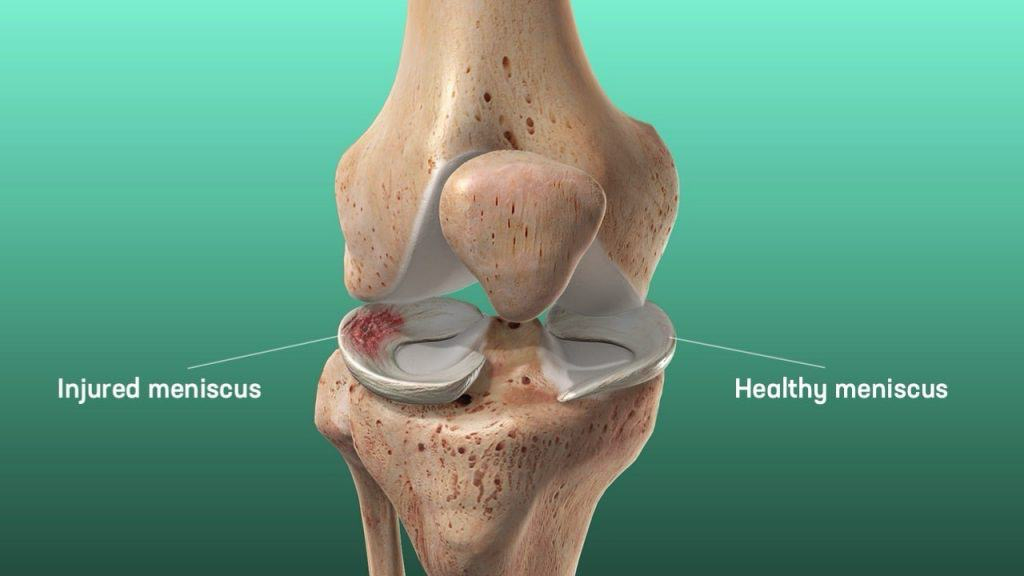
The knee joint has two menisci—the lateral meniscus and the medial meniscus. The lateral meniscus is smaller, circular, and O-shaped, while the medial meniscus is C-shaped, broader, but thinner with a flat underside. The medial meniscus is wider at the back than the front and is firmly attached to the tibia, joint capsule, and tibial collateral ligament by coronary ligaments.
For those looking for best meniscus repair surgery , Dr Nitin Rawal and his team at AOSC specialize in advanced techniques to ensure optimal recovery and long-term knee health.
Along with meniscus repair, they also offer expertise in shoulder arthroscopy and other joint procedures for complete orthopedic care.
The lateral meniscus is loosely attached to the tibia and joint capsule, with a strong connection to the popliteus tendon at the back. Its front part merges with the ACL, and both menisci are linked by the transverse ligament in front of the ACL.
Functions:
- Load Distribution: Helps spread weight evenly across the knee by improving joint fit.
- Shock Absorption: More elastic than cartilage, it absorbs impact and supports 50% of weight in extension and 85% in flexion.
- Stability: Deepens the tibial surface and acts as a secondary stabilizer, especially important after ACL injuries, where the medial meniscus plays a key role in preventing excessive forward movement of the tibia.